
Knee Arthritis & Management
What is the Knee Joint?
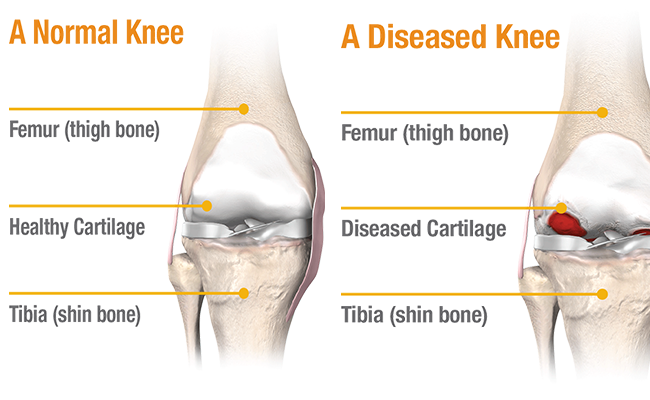
The knee joint is composed of three separate bones. They are the lower end of the thigh bone (the femur), the upper end of the shin bone (the tibia) and the knee cap (the patella). These three bones are joined together in a loose arrangement by a surrounding capsule. In addition, there are special ligaments which blend with the capsule outside the knee and provide additional reinforcement. In particular, there are medial and lateral ligaments which help stop the thigh bone and the shin bone from moving sideways upon each other. There are also ligaments inside the knee joint. In particular, there are the anterior cruciate and the posterior cruciate ligaments. These ligaments provide stability in a frontwards to backwards direction, and also provide rotary stability. There are two cartilages or menisci within the knee. These serve to increase the surface area for load distribution, act as cushions or shock absorbers between the femur and the tibia. A normal joint contains between 0.5ml and 2ml of fluid. The knee joint is special in that the bones can hinge, glide and rotate. The joint surfaces are covered with hyaline cartilage.
Arthritis
A smooth, slippery, fibrous connective tissue called articular cartilage acts as a protective cushion between bones inside the joint. Arthritis develops as the cartilage begins to deteriorate or is lost because of wear and tear as part of aging or because of disease like Rheumatoid arthritis. As the articular cartilage is lost, joint space between the bones become narrow. This is an early sign of osteoarthritis and is easily seen on X-Rays. The synovium (a membrane that produces a thick fluid to nourish cartilage and keep it slippery) becomes inflamed and thickened. It may produce extra fluid that causes additional swelling. Slowly over time bone ends rub against each other and wear away. This results in the deformity of the joint. Normal activity becomes painful and difficult. Pain can even interfere with simple daily activities.
Common symptoms of arthritis include pain, stiffness, loss of joint motion, swelling, cracking sounds and changes in the shape or deformity of affected joint
Who develops arthritis?
- Knee arthritis typically affects patients over 50 years of age but may affect younger patients too
- It is more common in patients who are overweight, or suffering from Rheumatoid arthritis or Ankylosing spondylitis. In some patients arthritis tends to run in families.
- Other factors that can contribute to developing knee arthritis include injury to the knee, and fractures to the bone around the joint.
What is the treatment of knee arthritis?
- Non operative approaches : These include a reduction in body weight, anti-inflammatory analgesic tablets supplements (Collagen compounds, Diacernin, Glucosamines, Chondritin etc.), physiotherapy, the use of a splint, the aid of a walking stick or crutches for ambulation, the use of a wheelchair and modification of the usual activities of daily living.Other non-operative measures include the injection of cortisone (Steroid) compounds into the knee joint or the injection of artificial lubricants within the joint.The cortisone can serve to dramatically reduce the inflammation within the joint and may provide significant patient comfort. Unfortunately, these cortisone compounds (steroids) can have a deleterious effect on the cells that repair the cartilage surfaces, weaken bone and decrease resistance to infection. The artificial lubricants / Visco-supplements (Hyaluronic acid) may be useful in early stages of arthritis to relieve symptoms for variable period. The response to injections of this nature is quite variable and rarely is long-term symptomatic relief provided. In general terms, these forms of injection therapy should be restricted to patients in very special situations.
- Operative options:There are many operative options available for patients with arthritis of the knee joint. It should be appreciated at the outset however that all orthopaedic conditions should be first managed non operatively. Indeed, operative measures should only be employed if there are specific indications.One such indication in arthritis of the knee would be a failure of the patient to respond in an appropriate symptomatic manner to an exhaustive non-operative therapeutic regimen.
- Osteotomy : Patients who have a deformity as a result of arthritis of the knee are often excessively loading the diseased part of the knee. Every step they take, every move they make, the patient is aggravating the underlying arthritic problem. The rationale behind the osteotomy is to correct the deformity and redistribute the load bearing forces onto a better-preserved part of the knee joint itself.High Tibial Osteotomy is beneficial in early stages of osteoarthritis as the biomechanical forces are redirected; yet the patient maintains his or her own knee joint. The aim of this operation is to buy more time or useful miles from the joint before considering some form of knee joint replacement surgery.
Who need a knee Replacement?
If your answer is yes to most or all the questions, you probably are a candidate for knee replacement surgery
- Does severe knee pain limit your activities? (walking, climbing stairs, getting in and out of chair)
- Is your knee often swollen, not responding to medications or rest?
- Are your knees deformed?
- Are your knees stiff, which makes it difficult to bend or straighten?
- You dont get satisfactory relief from pain killers and other conservative methods?
Unicondylar Knee Replacement / Partial Knee Replacement
Unicondylar replacement or Partial replacement can be considered if only the medial or inner compartment of knee is severely damaged and the other compartments, Patella and Ligaments are well or fairly preserved. Recovery after Partial Knee Replacement is expected to be faster than after Total Knee Replacement. During Partial Knee Replacement Procedure, A total Knee Replacement implant is kept on standby incase the lateral and the patellar compartment or Anterior Cruciate Ligament are found damaged.
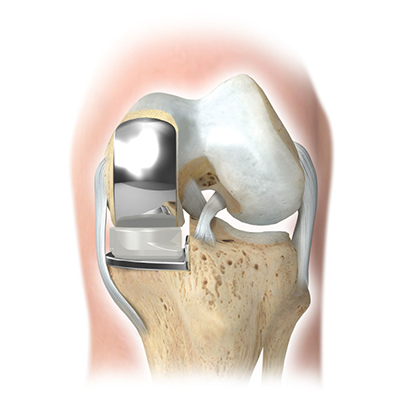
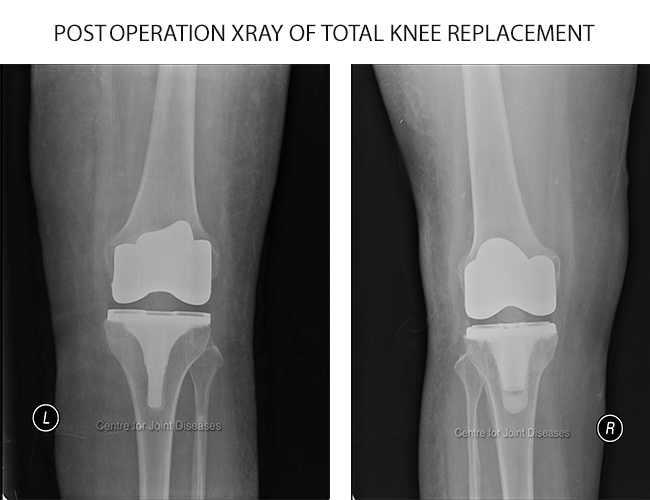
Total Knee Replacement
This is indicated for patients who have severe multi-compartmental arthritis, and who are unable to tolerate the ongoing discomfort despite application of all of the non operative therapeutic measures described above.
Procedure
Knee joint is exposed using a midline incision on the front of knee. Joint is exposed after separating the muscle and cutting through the capsule. The worn and damaged surface of bone and cartilage from lower end of femur (thigh bone) and upper end of tibia (shin bone) are removed and shaped to accept the prosthetic metal implants. A plastic spacer is again inserted between these two components. The soft tissues around the knee are carefully balanced to correct the alignment of the joint and optimize the function of knee
Realistic expectations
- Ultimate goal of knee replacement surgery is pain relief and improved knee function.
- Knee replacement surgery will not treat pain arising from other joints or back.
- Restrictions like avoiding running, high impact aerobics and sports like tennis are to be practiced for rest of life.
- Extreme bending, squatting and sitting cross-leg should be avoided to prevent dislocation and wear or early loosening of implants.
- Knee replacements last many years, but may need revision surgery when they wear out or loosen.
- Some Patients experience numbness or paresthesia on outer aspect of knee after surgery.
- Discomfort and swelling may take some months to disappear.
Points to remember after total knee surgery
After knee replacement, certain important aspects of your recovery need to be kept in mind:
- Walking and limited post-op exercises are important and should be performed as instructed by your physiotherapist. These have to be continued lifelong.
- Balance rest and activity, especially early in your recovery.
- Follow instructions to prevent clots.
- Know the signs of infection.
- Be careful and avoid falls.
- Carefully adhere to restrictions.
- Specific precautions to prevent dislocation of hip are available as separate documents.
Getting ready for the surgery
As with all operative endeavors, there is a list of potential pitfalls, problems or complications. To name a few there is risk of Infection, clots forming in the veins of the leg travelling off to the heart and lungs, compartment syndrome and loosening. Postoperative stiffness and swelling of the joint can also be problematic. All the precautions are taken to minimize the risk of complications.

Dr. Aman Dua
M.S. Orthopedics (AIIMS, New Delhi), D.N.B. Orthopedics, M.N.A.M.S., P.G.D.H.M.
Director - Joint Replacement
Fortis Escorts Hospital, Delhi

