
High Tibial Osteotomy : Description
HIGH TIBIAL OSTEOTOMY
Introduction
The tibia is the shin bone, the upper part of which forms half of the knee joint. The word osteotomy refers to the division of the bone. A high tibial osteotomy therefore refers to the division of the upper end of the shin bone just below the knee. The gap thus created is opened up and stabilized, allowing realignment of the limb. The overall aim of the procedure is to biomechanically unload a diseased compartment of the knee joint and more appropriately and equitably distribute the weight bearing forces onto the better-preserved compartment of the knee joint.
What is It For?
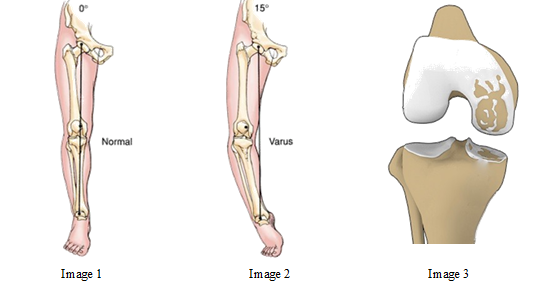
Image 1 and 2 shows a front-on view of a pelvis with two lower limbs attached. Imagine that you are looking at a patient front on. The line connecting the centre of the hip and the centre of the ankle represents the forces dictated by gravity when you are standing on one lower limb. The image on the left (image 1), you will note that the line passes exactly through the centre of the knee joint. This therefore results in the application of equal forces to both the medial and lateral (or inside and outside) compartments of the knee joint.
On the right image (image 2) the line representing the force of gravity, connecting the centre of the hip to the centre of the ankle passes well medial to the centre of the joint. The diseased medial compartment is therefore being excessively loaded and degenerates further (Image 3). Only a small portion or none of the weight bearing force is being applied to the better-preserved lateral compartment.
The essence of the high tibial osteotomy is to realign the shin bone, restore the normal valgus angulation and allow the weight bearing forces to be more properly redistributed to the better preserved lateral compartment.
How is It Done?
You will be admitted to hospital possibly the day before the operation or alternatively, on the day of surgery. Details concerning your past and present medical history will be entered onto your own personal clinical record. Your lower limb will be shaved. It is important that you bring your x-rays to hospital with you.
Procedure is generally performed under regional anaesthesia. During surgery straight incision will be made over the inner aspect of your knee extending for a short distance down inner aspect of your shin bone. The underlying upper end of the shin bone is exposed. Special drills and guides are used with the aid of a special x-ray machine that can image the region in question. A wedge of bone with a lateral base is removed from the upper end of the shin bone. Pins are inserted obliquely into upper part of the shin bone from inner aspect to outward direction under x-ray monitoring. After confirming the position of pins, bone is cut with a saw under x-ray view. Now the bone cut is opened gradually to create a predetermined triangular gap (Image 4) with special instrument to correct the limb alignment. The gap so created is stabilized with plate and screws (Image 5). A postoperative x-ray will be performed.
Antibiotics and pain medicines are administered in peri operative and postoperative period.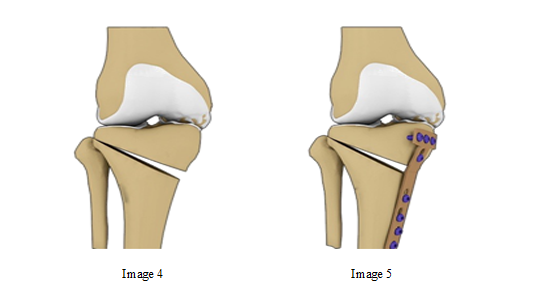
Physiotherpy and Mobilization
On the first postoperative day, the team physiotherapist will instruct you about special muscle exercises and assist with your mobilisation with crutches. You are allowed to walk without putting any weight or toe touching on the operated leg for the period of 6 weeks. During this period, you are expected to do muscle strengthening exercises and gradual knee bending as advised by surgeon and physical therapist. You can expect to be discharged on the second or third postoperative day.
Sutures are removed after 2 weeks of surgery. We see you again at six weeks postoperative stage and new x-rays will be done. If healing has progressed satisfactorily, you are allowed to gradually increase the weight on the operated leg. We would expect you to regain near normal function in next four to six weeks.
Potential Risks and Complications
Potential risks and complications include infection (about 1%), a delay in healing of the osteotomy or a fracture from the osteotomy site up into the joint, injuries to the surrounding nerves and blood vessels. Clots can form in the veins and travel off to the heart and lungs. There are also risks associated with general anaesthesia. Anaesthetic risks can be discussed with the anaesthetist at the time of your pre operative consultations.
The End Result
The advantage of a tibial osteotomy over a total knee replacement is that you have retained your own knee. The arthritis still resides within the joint and therefore you can expect some ongoing discomfort following the surgery. A tibial osteotomy matures with time. Then best results are usually achieved some ten to twelve months post operatively. Ideally, those good results are maintained for six, eight or even ten years. At that juncture, it may be useful to ultimately undergo a total knee replacement. The essence of a high tibial osteotomy is that it is designed for younger people, to buy some time before undergoing a knee replacement. Should you have any further questions or concerns about this procedure, you should feel free to discuss them with me at any time.

Dr. Aman Dua
M.S. Orthopedics (AIIMS, New Delhi), D.N.B. Orthopedics, M.N.A.M.S., P.G.D.H.M.
Director - Joint Replacement
Fortis Escorts Hospital, Delhi

